The Shoulder in Ankylosing Spondylitis
Introduction
Shoulder joint involvement is a common features of AS but it does not generally cause the same degree of disability as spine or hip involvement. The medical knowledge relating to shoulder involvement in AS is limited in comparison to the spine.
Review of Shoulder disease in AS
In an excellent Canadian study, a chart review of 400 AS patients and 285 controls was undertaken. Thereafter, MRI scanning was performed on 15 AS patients and in 91 patients where the cases had nonspecific shoulder pain.
The study showed that shoulder pain was recorded in 3.5% of patients by chart review. However, shoulder involvement was evident in nearly 25% of AS patients when they were examined by a doctor who was specifically looking for shoulder problems. This points to an under recognition of shoulder disease in AS.
Acromioclavicular joint (ACJ) arthritis
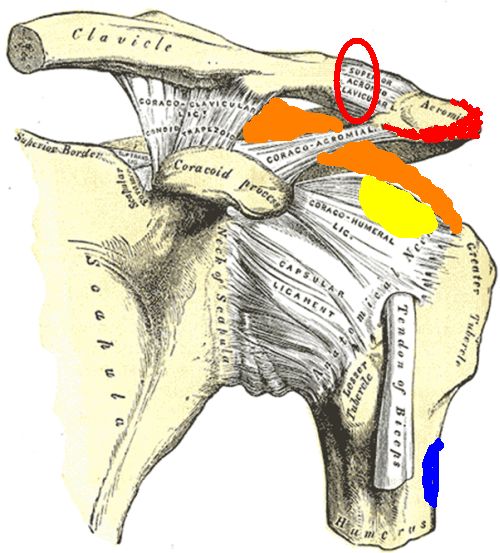
Acromioclavicular joint (ACJ) arthritis was the most common lesion observed in AS shoulders, but was also common in the non-AS group. The ACJ is actually outside of the shoulder. This is important as ACJ pain is felt in the shoulder and a local steroid injection may be highly beneficial if placed at that site. The site of the ACJ is shown inside the red circle in the figure below.
|
| The acromioclavicular joint is on top of the shoulder and links the shoulder to the outer part of the collar bone (LOCATED INSIDE THE RED CIRCLE). This is a fibrocartilagenous joint and is a common site of disease in AS |
Rotator Cuff Tendonitis
Rotator cuff tendinitis was commoner in AS patients than in controls. This included abnormalities of the supraspinatus tendon, infraspinatus tendon and subscapularis tendon.
Bone erosion in the Shoulder
Bone erosion of the greater tuberosity of the shoulder at the supraspinatus tendon insertion with or without adjacent bone oedema was also a feature of AS. This abnormality occurs within the enthesis organ of the supraspinatus tendon, where the tendon compresses the bone. So erosion formation in the shoulder in AS is linked to the enthesis organ. The tendon is shown in orange and the site of erosion in yellow.
Deltoid Enthesitis
Intense acromial entheseal oedema at the deltoid origin was observed only in AS shoulders. Of special note, no abnormalities were evident at the deltoid muscle insertion. The red shadowing shows the site of bone oedema at the deltoid enthesis origin in the Figure. The deltoid insertion where no erosion occurred is shown in blue. These differences are linked to the mechanics of the deltoid insertion which is located well away from the joint and where fibrocartilage is absent (see two types of entheses).
|
|
The common pathologies linked to AS shoulder disease are shown
|
Medical Considerations
Shoulder pain in a patient with AS may be due to mechanically related or degenerate related enthesopathy rather than inflammatory enthesitis. The first two groups may not respond to therapies that are effective in AS.
Local steroids injections should be effective if placed in the correct place.
For resistant cases biological therapies may be effective. It is likely that these will be prescribed if the patient also has active spinal disease.
References

Resources
Health Service Executive Causes of shoulder pain.
National Institute of Arthritis and Musculoskeletal and Skin Diseases What Are Shoulder Problems?