Microscopic Inflammation in Normal Insertions
Introduction
All parts of the enthesis including the bone and fibrocartilage are prone to injury. The resulting microdamage to the enthesis structures must be repaired to avoid complete failure of the skeleton. The first stage of repair involves removing damaged tissues or microscopic debris.
Damaged tissue is removed by an inflammatory reaction. This is carried out by cells of the immune system including macrophages which literally means "big eaters". When the debris is removed the same immune cells can switch off the inflammation and set in train a tissue repair process.Examples of Micro-inflammation
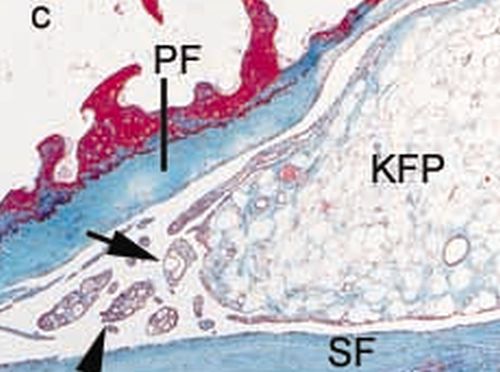
This image below shows microscopic overgrowth of the synovium in the synovio-entheseal complex [1]. These changes to the synovium adjacent to the enthesis are associated with inflammation. This removes damaged tissue.
|
| This shows microscopic thickening of the synovium in the enthesis organ. The arrowheads show the
overgrown synovium which is termed synovial hyperplasia. This tissue has lots of infiltrating macrophages.
SF and PF = sesamoid and periosteal shock absorbing fibrocartilages. KFP= fat pad
|
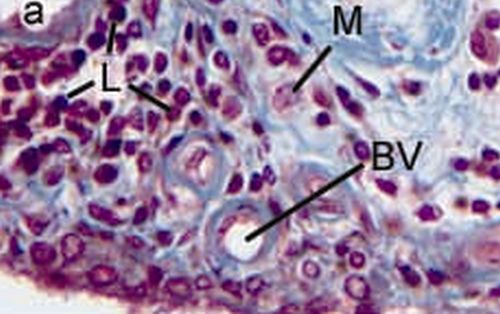
Quite florid microscopic inflammation may develop at the insertion site. This is depicted on the image below where there is lots of macrophage infiltration.
|
| This shows micro-inflammation at a normal knee joint enthesis.
M = macrophage which is a type of cell that removes damaged tissue and starts the repair process
L = lymphocyte which is another type of immune cell
BV= Blood vessel
|
To summarise, these inflammatory changes are taking place all the time as part of normal tissue repair at the enthesis and bone. It is thought that such microscopic changes don't cause symptoms as far as medical scientists currently know but this is an important area for research.
Implications
Inflammation doesn't go away but must be switched off. A genetic defect in switching off inflammation might be linked to chronic persistent inflammation developing. There is emerging genetic evidence for the failure to switch off inflammation being linked to some types of Spondyloarthropathy including Psoriatic Arthritis.
The role of inflammation at the enthesis in sports related pains is poorly understood. A defect in the magnitude of inflammation may be linked to tissue non-repair after chronic injury. This is an area ripe for research.
Whether microscopic inflammation may contribute to entities including overuse syndromes including work related upper limb disorders is difficult to prove due to the difficulty in getting enthesis tissue.
In some cases of mechanical enthesopathy it may be that drugs that suppress inflammation such as steroids may actually retard the normal repair process. Care is needed not to suppress the normal healing reactions.
References

Resources
Linus Pauling Institute Two Faces of Inflammation
Encyclopaedia Britannica Chemical mediators of inflammation