Osteoarthritis related Mechanical Polyenthesitis in a patient with a history of guttate psoriasis
Background
This case illustrates the importance of keeping an open mind in the assessment of cases with enthesitis or enthesopathy.
Enthesitis means that the primary problem at the insertion is related to inflammation.
Enthesopathy indicates that the primary problem is due to degenerative problems, "wear and tear" or other causes of pain where the dominant pathology has little inflammation evident.
The case below shows how an arthropathy that looked like Psoriatic related enthesitis initially settled to a more classical degenerative pattern of disease within 12 months.
Establishing the correct diagnosis is important so that patients are not offered inappropriate treatment.
The patient history
A 44 year old nurse presented with severe right elbow pain and loss of function.
This gradually evolved over a few weeks.
The patient had tenderness and swelling of the right elbow indicative of tennis elbow.
The patient also had pain in the small joints of the feet without stiffness and without swelling.
There was a history of guttate psoriasis 10 years earlier. This occurred following a streptococcal throat infection.
Her inflammatory markers including C-reactive protein were normal.
Paracetamol, codene and ibuprofen did not control her symptoms.
She was given an intramuscular injection of methylprednisolone 120mgs.
This helped her symptoms but her elbow remained painful.
She was booked for an ultrasound scan which was done 3 weeks later.
By this time the scan showed minimal inflammatory changes and patient remained stable on simple analgesia and was able to work.
A probably diagnosis of Psoriatic Arthritis was made.
How things developed
At 6 months the patient reported new development of constant pains about the left elbow.
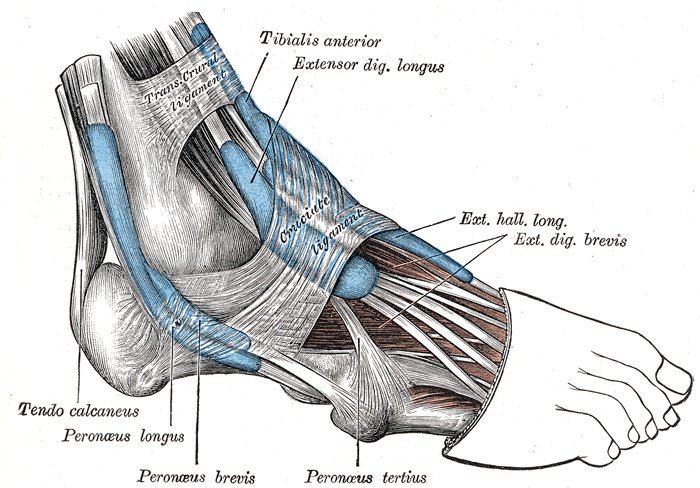
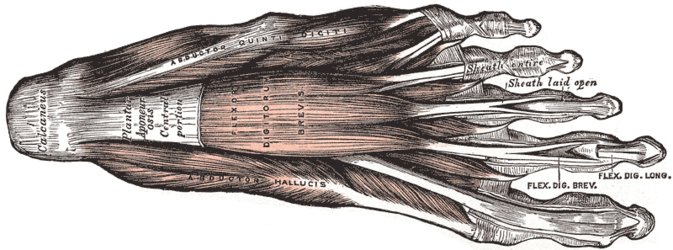
She also had constant pains in the left heel.
She had also developed pain on the outside of the right foot.
All of these locations were tender on pressure and on stressing of the relevant tendons.
 |
 |
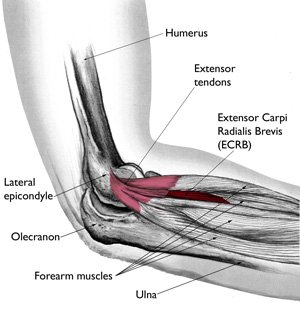 |
The patient had pain and tenderness over the 3 entheses as circled. These are common sites where it is easy to identify enthesopathy. In this case the diagnosis was therefore straightforward. However, enthesoapthy is often present at inaccessible sites e.g. deep within the neck of spine or within joints and cannot be confirmed by an examining doctor. However, a knowledge of the invovled sructure allows the doctor to delineate enthesoapthy. This image modified from The Body Almanac. © American Academy of Orthopaedic Surgeons, 2003. |
The patient reported that her mother had a history of generalised hand osteoarthritis.
The patient also reported that her periods had become irregular.
There was not joint swelling of spinal pain.
There was no current psoriasis or nail disease.
The clinical picture was therefore of mechanically induced or degenerative enthesopathy in a patient with a history of guttate psoriasis.
The management plan included activity and keeping weight down, physiotherapy for stretching exercise and podiatry assessment with insoles for the plantar fascia pain.
Failing these measures local cortisone injections would be a useful treatment option for short term pain alleviation.
Case summary
It is important to keep an open mind.
Psoriatic Arthritis and some forms of degenerative arthritis affect the same entheses regions.
With time the correct diagnosis of non Psoriatic related enthesopathy may become clear.