Enthesitis and Chest Pain in Ankylosing Spondylitis, Psoriatic Arthritis, Psoriasis and the Related Spondyloarthropathies
Introduction
The chest wall is an incredibly complex region with multiple insertion points that may become inflamed in Ankylosing Spondylitis and related disorders.
The purpose of this page is to explain to both patients and doctors why chest wall enthesitis is frequently not recognised, dismissed or misdiagnosed as heart attacks (myocardial infarction), angina, pleurisy or lung clots (pulmonary embolism).
Chest wall enthesitis is often of short duration and the outcome is usually good so its correct recognition is crucial to avoid unnecessary investigations and treatments.
Although chest wall enthesitis often occurs in cases with established Ankylosing Spondylitis or Psoriatic Arthritis, it can the presenting feature of arthritis in patients with undiagnosed chest pain including in psoriasis cases and the early phases of Ankylosing Spondylitis or related conditions.
Relevant Anatomy
Multiple insertions are present around the chest. Each rib has 3 different layered muscle insertions that run circumferentially around the chest wall. Enthesitis at these sites is very difficult to clinically locate at the time of examination.
The costo-sternal joints link the ribs to the breastbone. This is a common site of enthesitis and is often associated with tenderness (red areas).
The ligament and tendon insertions of the collar bone also join the breast bone and this can result in anterior chest wall pain.
Pain relating to the muscles of the abdomen insertions and the diaphragm insertion into the rib cage can also lead to chest pain. This may be associated with tenderness along the lower border of the rib cage.
The pain may also start at the spinous processes of the vertebrae (blue area). This is easier to diagnose as tender spots can be located when the physicians.
Enthesitis originating at the back of the spine may start in the vertebrae or the joints between the ribs and the vertebrae. This cannot be easily localised by the examining physician.
The ribs are also joint to the vertebrae at specialised joints called the costo-transverse joints which are also sites of possible enthesitis related pain.
Another possibility is that enthesitis is linked to inflammation of tendon or ligament insertions around the shoulder blade (scapula).
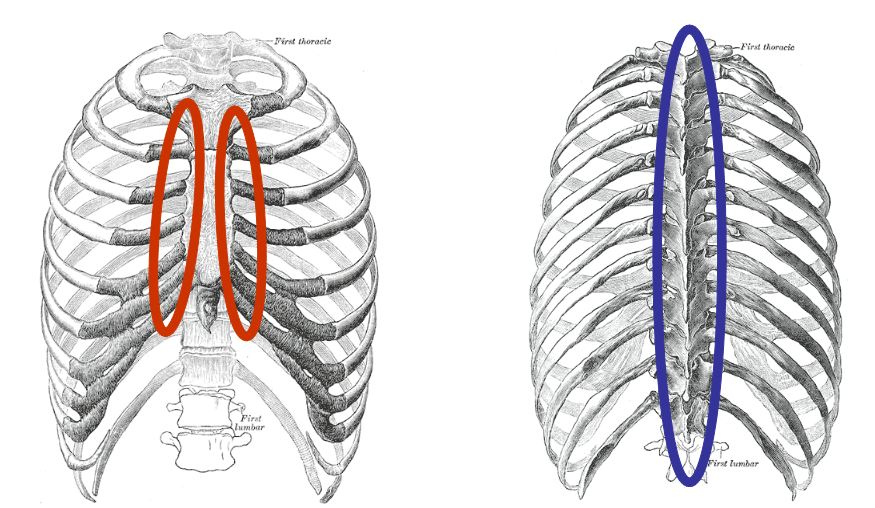 |
| This is an image of the rib cage from the front and from behind. There are numerous muscles attached between the ribs and numerous muscles and ligament insertions around the rib cage including those related to head and neck, arms and abdomen and diaphragm. Consequently it can be very difficult or impossible to find exact location of enthesitis. If it is possible to find exact spot of enthesitis in front of chest it is often within regions in red circles and painful spots can be injected if pain is chronic. The blue area represents sites of enthesitis that can readily be felt from the back of the spine. |
Diagnosis of Chest Wall Enthesitis
Symptoms are typically associated with stiffness that is worse in the morning and often improves as the day goes on. In some cases the pain can be pretty constant.
Symptoms may be aggravated by certain movements or by breathing, sneezing or coughing.
Symptoms may improve with anti-inflammatory tablets.
Given the anatomical complexity of the chest wall it is possible that the examining doctor may not be able to locate a specific site of enthesitis.
A careful examination of the head and neck, cardiovascular, abdomen and respiratory system should be performed to exclude problems at these sites.
The physician should examine the entire chest wall and adjacent tissues for tenderness or swelling.
It is easier to demonstrate tenderness along the sternum and rib joints but it can occasionally be demonstrated at other sites including the ribs and spine (red and blue areas).
Diagnosis
The diagnosis is often clinically based.
For severe or persistent symptoms other test are ordered.
For isolated enthesitis of the chest wall x-rays are often normal.
Blood tests that measure inflammation including CRP and ESR may be normal.
A bone scan (scintigraphy) may show increased uptake in the chest wall but this too can be normal.
Magnetic Resonance Imaging may show entheseal soft tissue and adjacent "bone oedema" (bone inflammation).
Given the complexity of the chest wall and the other important organs that can become diseased including chest and heart, it is crucial that patients seek medical advice to establish the correct diagnosis. This page offers educational pointers for patients to facilitate them in seeking medical advice.
Treatment
Simple analgesia including Paracetamol for mild cases.
Non-steroidal anti-inflammatory drugs also alleviate symptoms.
If the exact location of enthesitis can be localised then a local steroid injection can be very helpful.
If the chest wall enthesitis is part of a more generalised form of enthesitis such as Ankylosing Spondylitis or Psoriatic Arthritis then oral treatments or injectable drugs could be used.