Why did my Ankylosing Spondylitis start in the Sacroiliac Joint?
Introduction
Ankylosing spondylitis (AS) typically starts with low back pain in the sacroiliac joint. This page helps explain why ankylosing spondylitis starts in the sacroiliac joint.
The sacroiliac joint is mostly a fibrocarilagenous joint that is subject to high mechanical stressing. It shares anatomical, biomechanical and structural features with entheses. In common with entheses, the sacroiliac joint also shares an identical pattern of inflammation in the underlying bone which is termed osteitis. Of note, some regions of the sacroiliac joint may contain the other type of cartilage that is termed articular cartilage.
Why ankylosing spondylitis may start outside the sacroiliac joint too.
Ankylosing spondylitis can start elsewhere with chest pain that may be misdiagnosed as a heart or lung problem but is actually due to enthesitis.
The disease may start with heel,foot or with knee pain and be diagnosed as "overuse injury" or "tendonitis". So the disease may only progress to involve the sacroiliac joint with time.
The unifying concept is that disease localises to bone underneath fibrocartilage. The bone at these sites subject to high mechanical stressing which can be predicted based on the presence of fibrocartilage at all these sites.
|
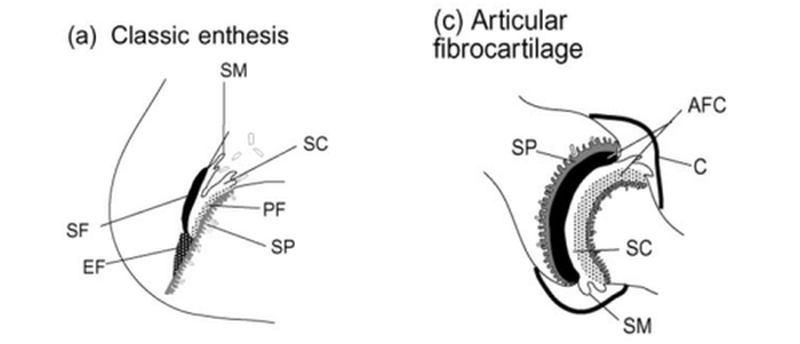
| This cartoon shows the similarities between an enthesis and the fibrocartilageenous joints including the sacroiliac joint. EF= enthesis fibrocartilage. PF= periosteal fibrocartilage. SF= sesamoid fibrocartilage. AFC= articular fibrocartilage that functions identically to EF, PF and SF. SC= synovial cavity. SM= synovial membrane or joint lining. SP= subchondral plate or bone plate underneath enthesis of sacroiliac joint fibrocartilage. |
|
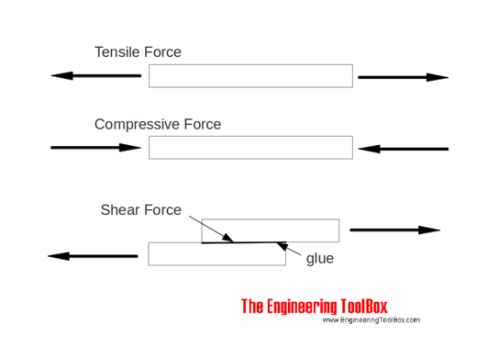
| This diagram shows the types of forces that act on both the sacroiliac joint and the entheses. We now believe that this explains the pattern of disease that patients with ankylosing spondylitis get. The particularly high stressing in the joint in young adults could account for the pattern of disease |
Other factors leading to disease of the sacroiliac joints in Ankylosing Spondylitis
We think that bone microdamage adjacent to fibrocartilage results in micro-inflammation which is a good thing and clears damaged tissue prior to repair. This is a bit like a dentist drilling out decaying tooth material before repairing the defect with a filling.
People with ankylosing spondylitis often have microscopic leakiness in the bowels that allow fragments of bacteria into the circulation. Such materials that are called adjuvants act as "smelling salts" to the immune system and likely make it relatively overactive. This may tip the balance in favour of a disease state in the sacroiliac joint and related tissues.
There is good evidence now to show that inflammation in the sacroiliac joint as measured by magnetic resonance imaging scanning is linked to abnormalities in the bowl in subjects who have no bowl symptoms at all.
Unfortunately the HLA-B27 protein picks up some self or bacterial components (or both) and then activates the immune system to magnify inflammation in the sacroiliac joint.
Specialised cells called T cells react to the HLA-B27-bound protein fragment complex and these cells can then carry the disease around the skeleton and especially to other sites in the spine.
Implications
There is no evidence that the fibrocartilage is defective in ankylosing spondylitis.
Given that HLA-B27 gene can protect people from the development of AIDs or Hepatitis C infection related liver damage, this argues strongly against the gene being defective.
There is evidence from experimental models of ankylosing spondylitis that normal levels of joint stress without injury is enough to trigger disease.
References

Resources
Ankylosing spondylitis (AS) Excellent Arthritis UK resource