Why does AS attack the Spine?
Introduction
Because Ankylosing Spondylitis (AS) has a tendency to start in the sacroiliac joint and because the initial inflammatory lesion may be located underneath the shock absorbing fibrocartilage, people have failed to realise the immense importance of the spinal entheses in AS. This page discusses the numerous entheses in the spine and how the presence of fibrocartilage at these attachment sites explains why AS may only involve the spinal column and spare the rest of the skeleton.
Many entheses in the spine
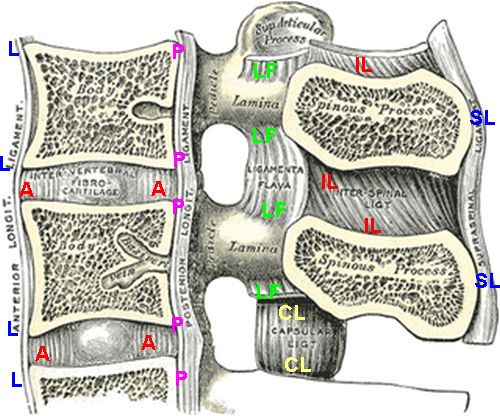
When one considers the ligaments that are shown in the diagram below there are more than 400 of these in the mobile part of the spine.
There are 23 discs with 46 anulus attachment sites above and below).
The anterior longitudinal ligaments contact each vertebral at its two corners (~46 insertions)
The posterior longitudinal ligaments contacts each vertebra at each corner (46 insertions).
The ligamentum flavum is located on both sides and makes 4 connections in total (approximately 88 attachments)
There are two facet joint capsules on each side each with 2 capsular entheses giving approximately 88 attachments
There is the interspinous ligaments between the spinous processes with two attached to each vertebra (44 attachments).
There is the supraspinal ligament with an attachment to each vertebra (22 attachments)
These are only the ligaments depicted in the cartoon below. In addition there are two ribs with 4 attachments to each vertebra (48 insertions).
|
A = annulus or disc attachment sites
L= anterior longitudinal ligaments
P= posterior longitudinal ligaments
LF= Ligament flavum
CL= capsular ligaments
IL= interspinous ligaments
SL= supraspinal ligaments
|
This is not counting the numerous tendon attachments of the numerous muscles around the posterior and anterior spine.
Other Anatomical Considerations
Compared to other joints the spine has many more entheses. The vertebrae are complelely made up of trabecular bone with the exception of the thin cortex. In children who develop AS it starts in the midfoot - another site of fibrocartilage and abundant trabecular bone. This difference between children and adults illustrates the key role of skeletal biomechanics.
Finally the spinal entheses are often very close to each other which may favour bony bridge formation and spinal fusion. Also the spinal entheses may not move in as many planes as peripheral entheses which could contribute to fusion also.
Given that AS affects the spine more than the peripheral skeleton and given that HLA-B27 is associated with inflammation in the bone adjacent to insertions this multiplicity of factors could be key to understand the curious pattern of disease.
Summary
Given that the immune system has access to all parts of the skeleton it seems likely that local tissue events that more commonly occur in the spine are key to AS disease localisation. The biomechanics and anatomy of the spine in conjunction with the HLA-B27 gene determine disease.