The Intervertebral Disc Enthesis
Introduction
The intervertebral disc forms an elaborate enthesis that links adjacent vertebrae together. What makes it different from other entheses is that it contains a gelatinous core that is a remarkable shock absorber. This core is reminiscent of a pressurised tyre and minimises stresses between the adjacent bone surfaces that makes the normal disc a remarkable piece of biological engineering. It is hoped enthesis biology knowledge on this website will help patients, doctors and scientists working on the disc better understand disease towards the aim of developing new research directions.
Anatomy
There are 23 discs in the human spine all of which can be affected by Ankylosing Spondylitis and the related Spondyloartropathies.
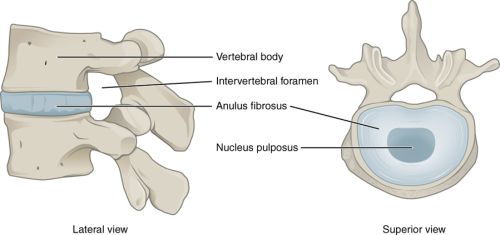
The intervertebral disc is composed of the anulus fibrosus (usually spelt as annulus fibrosus in literature) which is the tough outer ligamentous coat that is rich in fibrocartilage at its attachment sites to bone. The annulus is layered like an onion to give it extra strength.
The gelatinous core of the disc is called the nucleus pulposus which act like air in a pumped up tyre. This occurs because the specialised matrix in this region called glycosaminogylcans (GAGs) absorbs giving the disc its shock absorbing properties.
|
| This cartoon graphic shows a view from the side "lateral view" and a view from above which is take right through the middle of the disc. Of note the nucleus pulposus is well hydrated and acts like a the air in a pressurised tyre to keen the bones apart. The annulus circumferential enthesis functions like a tyre and keeps the disc in place. |
Blood supply of the Disc
At the attachment points to bone the enthesis is completely made of fibrocartilage. This resilient stress resisting tissue has no blood vessels that are friable and prone to injury.
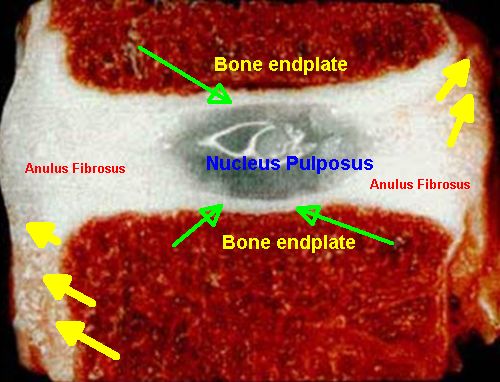
The vertebral endplate is bone and it is critically important in to function since the limited oxygen and nutrients that reach the core of the disc, to a large degree, do so via diffusion across this endplate [1]. The white regions in the figure below show the large extent to which a normal disc enthesis lacks blood vessels and the regions in red show where the blood vessels are located.
|
| This is an actual disc and beautifully shows to what extent the disc lacks a blood supply. The bony endplates of the vertebrae are red because they are highly vascular and contain blood. However the anulus fibrosus and the nucleus pulpous are completely avascular and appear as white. Fibrocartilage may also be present on the vertebral endplates where it dissipates stress from the compressed nucleus pulposus (green arrows). Finally only the outer surface of the ligament of the annulus has a limited blood supply (yellow arrows where the anulus changes from white to brown due to a limited blood supply |
Anatomy Considerations
The enthesis attachment point to bone and the nucleus pulpusos have no nerves in the healthy state.
Both early Psoriatic Arthritis and Osteoarthritis have a tendency to affect the discs in the neck. The discs in the neck are very mobile and show lots of age related damage in normal subjects. It is possible that microdamage to the neck discs is the common link as to why PsA and Osteoarthritis affect this site [2].
Degenerative disorders or "wear and tear" also typically affect the lower lumbar which manifests as pain which emanates from multiple tissues including bone bruising, new bone formation and scarring and nerve ingrowth to the enthesis.
The other problem that occurs in discs in a prolapsed disc which usually manifests in younger subjects when the jelly component of the disc protrudes backwards thru a tear in the annulus and compresses nerves typically leading to leg and foot pain. Prolapsed intervertebral discs may occur in younger people who otherwise have a fairly healthy disc.
Implications for back pain
Loss of the nucleus pulpusos material by allowing "bone on bone" compression may render the circular enthesis of the disc useless. Conversely damage to the anulus or to the bony endplate can lead to the nucleus pulposus being partially displaced into the bone which will also lead to loss of function.
Like other entheses around the body the disc enthesis is subject to microscopic fibrocartilage damage, microscopic bone damage, and abnormal vessel penetration in disease and nerve ingrowth that piggybacks on the blood vessels [2]. Given the body weight that is going through these diseased structures it is notoriously difficult to treat the resulting pain.
The engineering of the native disc is so complex that it is very hard to replace or repair. This is compared to the knee or hip joints where replacement is highly effective.
Beyond weight loss and smoking cessation, which may facilitate attempted repair responses, and consumption of pain relieving medications there is a lack of treatments for disc problems. Surgical procedures that fuse the diseased segment offer good pain relief. However, the altered mechanics tends to move the problem to the adjacent disc.
References

Resources
Chirogeek.com - an excellent resource on the intervertebral disc by Doug Gillard.