Missed diagnosis of enthesitis related arthritis
Subjects presenting with psoriatic arthritis (PsA) may have a delayed or a missed diagnosis because skin psoriasis may be absent. A careful search for enthesitis related pathology is necessary. This case illustrates a man misdiagnosed as gout who actually had PsA.
The patient developed intermittent ankle joint pain and swelling starting at age 36. He had disabling symptoms during disease flares and was diagnosed as gout 4 years later. He sees and orthopaedic consultant with knee pain. The exam was normal. An MRI scan shows subtle bone oedema in the patella and he was dischaged without a specific diagnosis.
He is referred to Rheumatology with recurrent ankle swelling. He reported that his father had psoriasis. At the time of assessment his ankle joint and knee joints were clinically normal. His history did not sound typical of gout.
He had 4 pits on third fingernail of the right hand and 2 pits in the 5th fingernail of his left hand and nail dystrophy in third toe or right foot. A review of his imaging supported the diagnosis of Psoriatic Arthritis.
 |
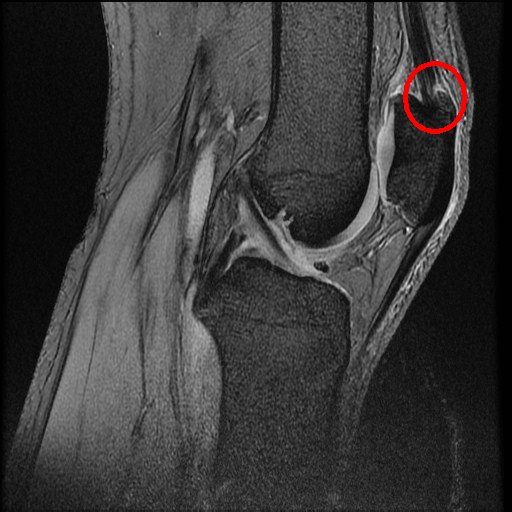 |
| x-ray from the time of orthopaedic assessment showed an enthesophyte in the right knee (circle). | MRI from that time showed the enthesophyte and adjacent soft tissue change and a normal knee otherwise (circle). |
This case illustrates how enthesopathy related pathology was mis-diagnosed as gout.
Lessons
- enthesitis related pathology may be intermittent.
- Patients may be normal at time of clinical assessment.
- the importance of the link between the nail and enthesitis related pathology needs to be looked for carefully.
- physicans need to be aware that new bone formation at insertions or MRI changes in young subjects may be clinically relevant.
- the level of awareness amongest radiologists and orthopaedic surgeons and even rheumatologists on how to recognise enthesitis related arthritis is limited.