Enthesitis, Enthesopathy and the Nail in Psoriatic Arthritis
Introduction
It has been recognised since the 1950's that nail disease is commoner in Psoriatic Arthritis than it is in Psoriasis [1]. This is surprising since, during development, the nail is derived from the skin tissues, rather than joint tissues.
It has also been shown that nail disease in subjects with psoriasis is a predictor for the future development of Psoriatic Arthritis [2].
Given that enthesitis may be the primary lesion in Psoriatic Arthritis lead doctors to carefully study the link between the nail and adjacent entheses. This has shown that the nail is inserted directly to the skeleton.
Anatomical linkage between the nail and the skeleton
The nail is intimately anchored to it by an elaborate network of entheses. These include:
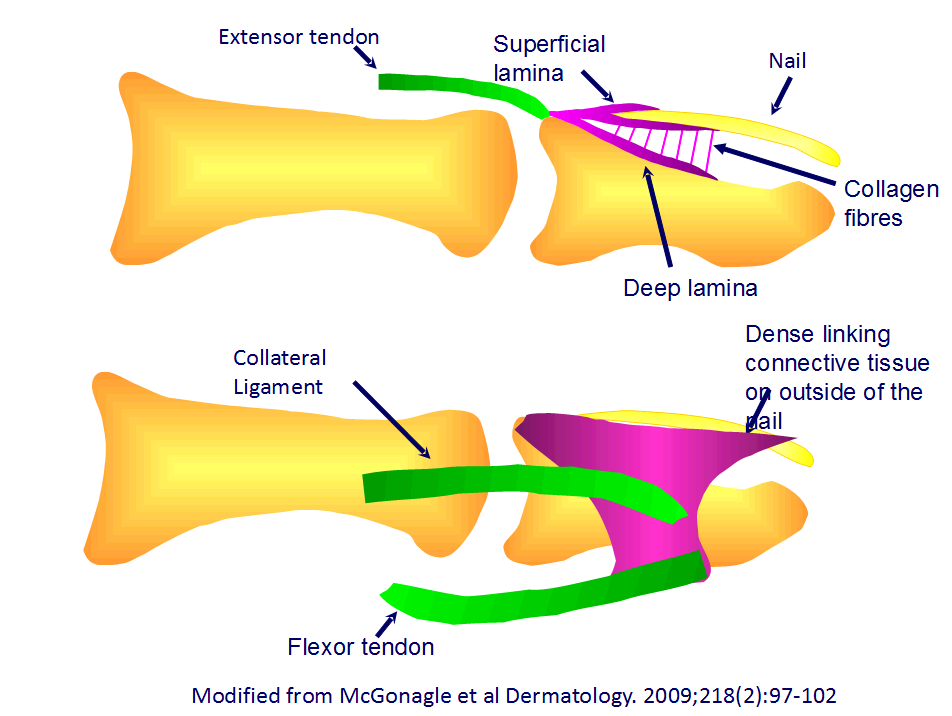
- Extensor tendon insertion directly to the nail [3].
- Fibres from extensor tendon run along the bone surface and the integrates with small structures called dermal ligaments that than anchor to the nail under surface [3].
- The ligaments which stabilise the finger joints (collateral ligaments) anchor to dense tissue at the nail margin to stabilise the outside of the nail to the sheleton [4].
- The flexor tendon on the opposite side of the bone to nail is indirectly anchored to the nail and helps hold nail tip down. This helps with grip strength during bending of fingers when the flexor tendon is taut.
 |
|
This cartoon shows the midline anchorage between the extensor tendon (green) and
the nail (upper panel). This is complex with additional small entheses linking the bone surface
to the underside of the nail. Secondly, near the outer margin of the nail there is also insertions
between thick reinforcing connective tissue and both the entheses of the flexor tendon and collateral
ligaments. This provides very strong integration of the nail to the skeleton.
|
Nail Disease and Enthesitis Considerations
It is noteworthy that the link between injury or trauma to the skin and joints has long being recognised as triggering factors in Psoriatic Arthritis [5].
There appears to be a link between nail disease in psoriasis with nail trauma or injury insofar that the dominant or most used nails are most often show changes [6].
It appears that an abnormal response to injury in the functional nail-joint unit may be key to understanding the link between nail disease and arthritis.
Basically the nail is the terminal extension of an enthesis network which is visible and is useful predicting other enthesitis related disease, namely Psoriatic Arthritis
The presence of nail disease in the fingers is also associated with enthesopathy at remote locations in the lower limbs [7].
Nail disease suggests that the psoriasis is more than skin deep and goes directly to the bone at other sites outside the nail.
Patients with psoriasis may get nail pain. The importance of nail related enthesitis as an underlying cause for this has not been determined thus far.
Nail Disease Treatment in Psoriasis and Psoriatic Arthritis
Nail disease has been a comparatively neglected area in psoriasis and Psoriatic Arthritis
Historically, dermatologists have used topical agents to treat nail disease. These have not been very effective.
This lack of effectiveness of topical therapies may relate to the deep connections between the nail and entheses that will not respond to this approach.
There is some evidence in Dermatology that local steroid injection or oral medications including methotrexate and cyclosporin may have utility for nail disease in psoriasis.
Modern systemic agents that are collectively termed "biologic therapy" have shown remarkable effectiveness for nail disease in psoriasis. These include the anti-TNF agents, infliximab, etanercept, adalimumab and golimumab and the anti-IL12/23 drug, ustekinumab.
More clinical research will clarify the precise role of enthesitis in nail disease in psoriasis and its role, in treatment outcomes.
References
