Lung Disease in Ankylosing Spondylitis
Introduction
Fortunately disease of the lung itself that causes significant damage that leads to shortness of breath is uncommon in Ankylosing Spondylitis (AS). The major way in which AS causes breathlessness is due to fusion of the entheses around the spine and ribcage which restricts breathing. This page explains why AS can affect the lung tissue itself and explains how the similarities between lung disease and enthesitis.
Mechanism
The mechanical link between enthesitis and the other manifestations of AS is shown in the figure below.
|
| In 2001 the shared common features of stress at the enthesis and stress at the lung apex was also suggested. Repetitive movements and mechanical stress and tissue microdamage at both sites is the best explanation for this pattern of disease at seemingly different tissues [1] |
The lung is very elasticated and collapse on itself so there is greater tension on the tissue at the apex. This tissue is in a state or repetitive movement and as such it is reminiscent of the entheses.
Thin tall people are prone to develop blebs or "blow out" bubbles in the lung apex. These are related to physical stress and can rupture and this is called a pneumothorax. This is completely different to AS related lung scarring which is termed fibrosis. But it shows how shared mechanical factors lead to disease at that site which is termed the apex.
What lung disease in AS looks like
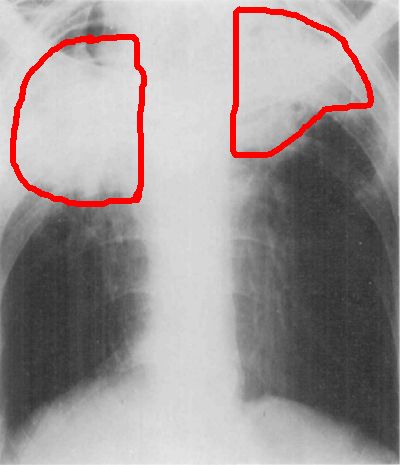
When AS affects the lung it is typically the top of the lung or the region behind the collar bone that termed the apex. The characteristic lesion is called apical fibrosis which is basically scarring at this site. As stated it is not a major clinical problem but can occasionally occur in AS.
|
| This is a chest X-Ray of a patient with AS. The area inside the red circles shows the scanning at the top of the lung [2] |
Symptoms
- Shortness of breath
- Cough
- Sputum production
- Coughing up blood
- Pleurisy of lung lining inflammation
- AS related areas of inflammation are prone to infection
A patient with AS should see their doctor if they have any of the above symptoms. Apical fibrosis is very uncommon and there are many more common causes of shortness of breath in AS.
Implications
As stated lung disease is not a big clinical problem. All patients should however refrain from smoking for two reasons.
First it directly damages the lungs.
Second it likely accelerates the ribs and spine fusion that decreases lung function.
References
