Shared Anatomy of Psoriatic Arthritis and Osteoarthritis
Introduction
This page explains the shared anatomical features of psoriatic arthritis (PsA) and some types of osteoarthritis (OA). Basically both may share a common anatomical site of disease origin at the enthesis. This can make it difficult to tell the two apart [1].
Mechanism
OA is regarded as a disease of "wear and tear" and joint injury is known to trigger it.
The role of injury or microdamage in PsA is also increasingly recognised.
The cartilage in the small joints is nearly always less than 1mm in thickness and sometimes in the region of 1/5 of a millimetre [2]. By contrast the ligaments and entheses in the small hand joints are much larger and can be in the region of 3mm thick. Wear and tear is likely to occur in these bigger structures.
|
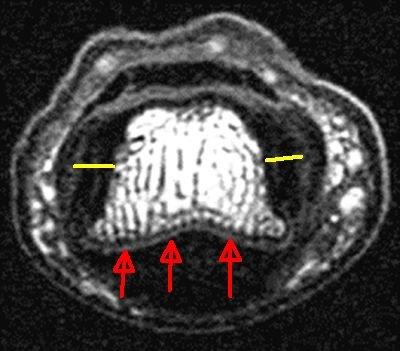
| This is a small joint of the hand viewed in cross section. The cartilage on the surface of the bone (grey colour) is comparatively thin (red arrows). However, the collateral ligament entheses are much thicker (yellow arrows). |
The thickness of the enthesis can also be viewed in other planes.
|
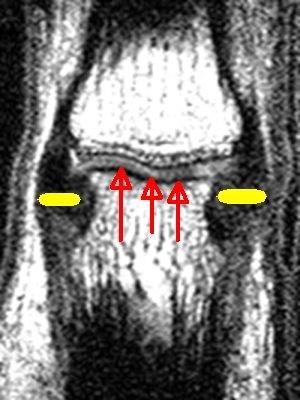
| In this image the relative thickness of the ligament enthesis is shown by the yellow arrows. The thickness of the cartilage covering the ends of the two bones (2 faint grey lines) is much less than an enthesis. The red arrows point towards the cartilage. The black immediately underneath the cartilage is the bone plate. |
Why are small joint entheses so big?
The reason for the large size of the small joint entheses is that they do more than just stabilise the hand joints.
If you fall over, your hand must take your whole body weight. If not, multiple dislocations, damage and loss of function would follow. So these entheses must accommodate the weight of the entire body when needed.

|
| The entheses in the small joints that are prone to both OA and PsA do a lot more than simply anchor the bones. They must be strong enough to take the entire body weight when one falls over. This accounts for why these small joint entheses are a lot bigger and thicker than joint lining cartilage. |
Unlike cartilage which is avascular the fact that blood vessels are closely related to the attachment site makes inflammation more likely when damage does occur.
The inherent risk of damage brings with it good powers of healing. It may also make excessive tissue repair reactions more likely.
Summary
Given that entheses are sites of high joint mechanical stressing and given that stress and injury is important in PsA and some types of OA, it is anticipated that both diseases may attack the same territory.
References
