Fibrocartilagenous Joints
Introduction
The entheses that are subject to inflammation in the Spondyloarthropathies (SpA) have a shock absorbing tissue called fibrocartilage at the bony attachment sites.
However, the SpA group of diseases also attack joints that are lined by fibrocartilage instead of the more common type of articular cartilage which lines most joints. Fibrocartilage is most notable in the sacroiliac joint where ankylosing spondylitis often starts.
Fibrocartilagenous joints are subject to compression, tension and shearing forces. These forces act not only on the fibrocartilage but also on the adjacent bone. An abnormal response to mechanical stressing is the common denominator between enthesitis and fibrocartilagenous joint disease. This page provides information about the other joints that may be attacked in the SpA group of diseases.
Fibrocartilagenous joints prone to The Spondyloarthropathies
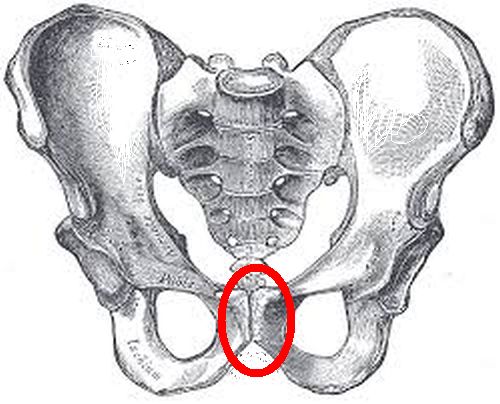
The Pubic symphysis
|
| The fibrocartilagenous pubic symphysis joint is inside the red circle. Disease of this location is common in Ankylosing Spondylitis and other Spondyloartropathies and also in athletes including footballers and rugby players |
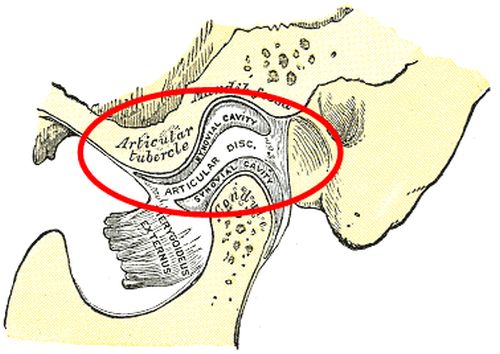
The Tempomandibular joint (jaw bone joint)
|
| Occasionally the tempomandibular joint can become involved in Spondyloarthropathy |
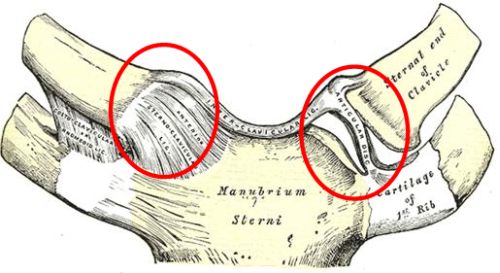
The Sternoclavicalar joint (breastbone attachment)
|
| Both sternoclavicular joints are shown in this image. Spondyloarthropathy at this location is often part of an entity called the SAPHO syndrome |
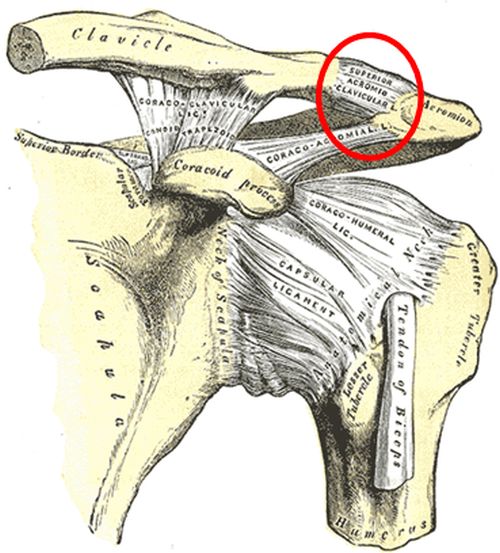
The Acromioclavicular joint (collar bone to shoulder joint)
|
| This joint sits on top of the shoulder (red circle). Spondyloartthropathy at this site is poorly recognised in our experience |
The joints of the midfoot
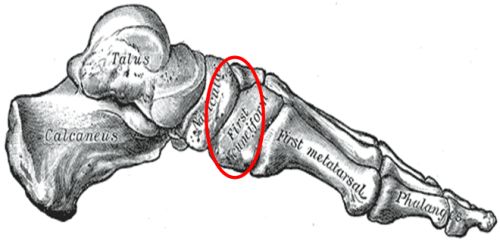
|
| Several bones in the midfoot are lined by fibrocartilage. This is probably why juvenile Spondyloarthropathy may start at this location |
The Sacroiliac Joint [link]
Implications
Inflammation of these joints results in diffuse bone marrow inflammation which is termed osteitis which is readily seen on MRI scanning. However, any of these joints can also become diseased due to infections known as a septic arthritis (centred in the joint) or osteomyelitis (infection centred in the bone).
We have seen isolated arthritis of these joints being investigated for infection which includes biopsy procedures. We have also seen patients being treated with protracted courses of antibiotics without any benefit.
Diffuse bone inflammation on scanning including MRI may resemble bone infection or osteomyelitis Diffuse bone inflammation adjacent to fibrocartilage which is a key feature of Spondyloarthropathy should be considered in people presenting with disease of the fibrocartilagenous joints.
Reference

Resources
See Anatomy of the Human Body for more detailed anatomy of the fibrocartilagenous joints. From the 1918 edition of Grays Anatomy.