Diffuse Idiopathic Skeletal Hyperostosis (DISH) - An AS mimic
Introduction
DISH is a chronic age related condition, with characteristic new bone growth at the entheses.
DISH represents the best example of enthesogenic osteoarthritis- a type of osteoarthritis that is exclusively related to the enthesis.
It may present as constant type pains in the neck or spine or in peripheral joints.
In some cases there may be minimal symptoms and the diagnosis is "incidentally" picked up on an X-ray.
It is not uncommon for DISH to be incorrectly diagnosed on x-ray as Ankylosing Spondylitis.
Clinical Features of DISH and telling it apart from Ankylosing Spondylitis
This can be extremely difficult especially in older patients who present to doctor for the first time.
Typically Ankylosing Spondylitis starts in the teenage years or early adulthood but DISH starts later.
Although early morning stiffness is more typical of Ankylosing Spondylitis it may also occur in DISH.
Alternating buttock pain that is more typical of Ankylosing Spondylitis may also occur in DISH
Painless reduction in joint movements may be evident as a result of the new bone formation in DISH
The blood tests that may be informative in Ankylosing Spondylitis including HLA-B27 status and C - reactive protein (CRP) or erythrocyte sedimentation rate (ESR) are either normal or negative in DISH.
In a minority of cases it can be virtually impossible to distinguish between Ankylosing Spondylitis and DISH.
Diagnosis of DISH
X-Ray assessment has been the "gold standard" for diagnosing DISH.
It is important to realise that DISH, Psoriatic Arthritis, and Ankylosing Spondylitis all affect the same anatomical territory i.e. the enthesis.
Some forms of Osteoarthritis which are less extensive than DISH also affect the enthesis and show extensive new bone formation.
Considerable judgement is needed to differentiate between DISH and Anklyosing Spondylitis in particular.
The following features are used to diagnose DISH [1, 2]:
- Flowing calcifications and new bone formation in the front parts of at least 4 vertebral bodies, with or without osteophytes (new bone originating at the enthesis).
- Preservation of disc height in the involved areas and an absence of excessive disk disease.
- Absence of bony union of the facet joints (small joints at back of spine) although narrowing and sclerosis of facet joints are acceptable
- Absence of sacroiliac erosion, sclerosis, or bony fusion that is typical of Ankylosing Spondylitis. When the joints are knitted together in DISH, this is due to bridging on the outside of the joint rather than through the middle of the joint as in Ankylosing Spondylitis [3]
Interesting Facts about DISH
Postmortem studies show that changes compatible with DISH are present in the skeleton in 10% males older than 65yrs
The disease is twice as common in men compared to women
Changes compatible with DISH are very common in ancient skeletons making DISH the oldest rheumatic disorder. Thus, the oldest arthritis is related to enthesopathy.
Although the bones are strong the loss of mobility at the entheses can be associated with fractures of the spine but this is not common.
Pathological Features
DISH is due to excessive new bone formation of the entheses.
It is important to realise that new bone formation occurs at the normal enthesis from youth to old age [4, 5]. Therefore, DISH represents an exaggerated tissue repair response.
Abnormal blood vessel responses in tissues at or adjacent to the enthesis might contribute to disease [6].
It is thought that specialised stem cells called mesenchymal stem cells may proliferate and form bone forming cells called osteoblasts at the insertions. This has not been studied in man.
DISH is associated with Type II Diabetes and obesity. Consequently, DISH has been associated with metabolic problems to increased sensitivity of bone progenitor cells at the enthesis to insulin and other growth promoting or "anabolic" chemicals [6].
Conditions that mimic DISH
Localised forms of Osteoarthritis:
- Spinal
- Peripheral
Spondyloarthroapthy
- AS
- PsA
Acromegaly
- Also associated soft tissue and cartilage thickening
- Shared hormonal influences with DISH including a chemical called Insulin like growth factor-1 (IGF-1)
Peripheral enthesopathy:
- Mechanical
- Hypervitaminosis A (excessive Vitamin A ingestion)
- Retinoid therapy for acne can cause entheseal pain
Treatment
In a sense DISH is the opposite of cancer. In cancer tissues are destroyed but in DISH new bone is formed at entheses.
Therefore DISH does not usually lead to loss of mobility or independence.
Complications of DISH should be sought out or anticipated. These are uncommon and include pressure from the new bone in the throat causing difficulty in swallowing or pressure on spinal cord or nerves causing weakness or loss of power.
The joint stiffness that is reported may simply reflect new bone formation partially encasing the joints and as a result medications may not help.
Physiotherapy to maintain mobility has a role.
The use of analgesia including paracetamol and codeine based analgesia may help.
Non-steroidal anti-inflammatory drugs may help but these are generally much less effective than in the enthesitis associated with Ankylosing Spondylitis.
In theory non-steroidal anti-inflammatory drugs might slow down new bone formation but given that these agents can be associated with heart attacks and bleeding ulcers they are best avoided where possible.
For bouts of focal enthesitis such as tennis elbow local steroid injections can be given.
For bouts of joint swelling, which is uncommon, steroid injection into involved joints may help.
Finally underlying medical problems including diabetes should be adequately controlled.
Case Illustrations
 |
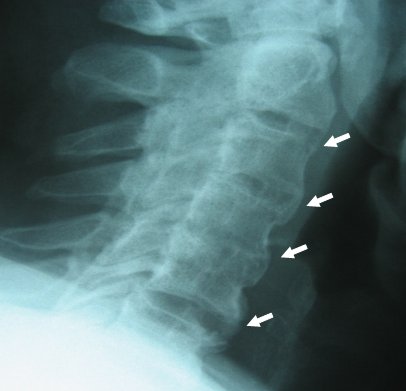 |
| Two examples of DISH with new bone formation in the next. In both cases the disc spaces are well preserved. Florid enthesal new bone formation in the left (4 white arrows). If these changes were confined to the neck only then the working diagnosis would be Cervical Spondylosis or Osteoarthritis. The image on the right shows florid new bone formation at the entheses of the neck in a 58 year old man with DISH | |
 |
|
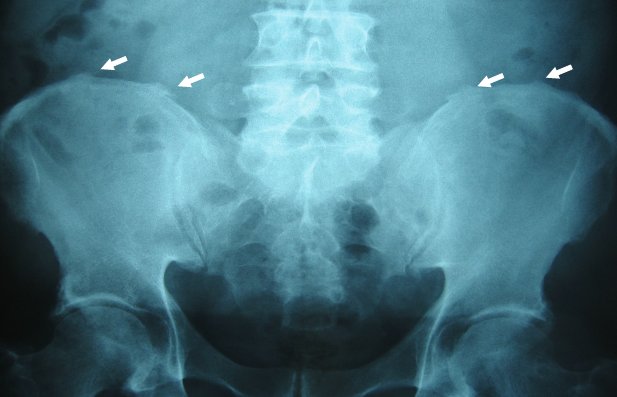
| This shows wisps of new bone formation at tendon/ligament entheses attachments to the Pelvis. This enthesopathy is usually not associated with pain |
 |
 |
| Early changes of DISH in spine with florid new bone formation at entheses. This disc spaces are well preserved | This case was labelled as DISH. However there is disc space loss and the new bone formation is not flowing in straight lines but is like a birds beak (arrowhead). This has occurred because of disc has degenerated initially and has partially collapse so the pattern of bone formation is different. This illustrates how the spectrum of DISH merges into the commoner garden variety of wear and tear or Osteoarthritis |
 |
X-ray specialists state that for a radiographic diagnosis of DISH to be made new bone formation to bridge 4 consecutive vertebral bodies in the thoracic spine (rib cage region). There must also be an absence of degenerative disc disease and the absence significant facet joint changes (red arrowhead shows a facet joint). On right image the new bone linked to enthesopathy is shown (white arrows) Essentially the discs spaces are normal (yellow arrowhead for disc space). | |
 |
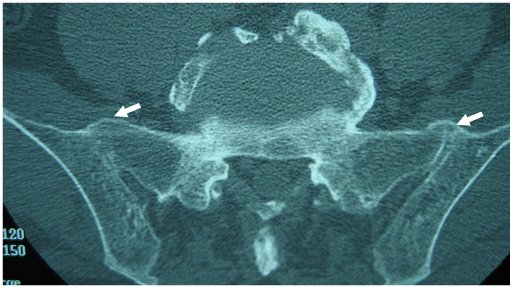 |
| At first glance the X-Ray on the left shows apparent fusion of the Sacroiliac joint (white arrows). The corresponding CT scan of the Sacroiliac joint on the right shows that the new bone formation is at the entheses only (white arrows). The joint space underneath is preserved in DISH as in this case but it is obliterated in Ankylosing Spondylitis. |
 |
 |
| New bone formation in DISH of the heel (left) and elbow (right) | |
References
